INTRODUCTION
It is known that anticipation consistency is a necessary link in the regulation of activity, behavior, and emotions.1 Based on the results of numerous studies, it can be argued that anticipation abilities as a whole are involved in the processes of personality adaptation to changing environmental conditions.2,3 Clinical, psychopathological, and experimental psychological studies have confirmed the role of violations of anticipation mechanisms in the etiology and pathogenesis of neurotic, psychosomatic disorders, and maladaptation of patients with personality disorders.4,5 It was revealed that the violation of the processes of anticipation, in turn, leads to a mismatch of the adaptation system, and, as a consequence, to maladaptive behavior.6
However, most of the issues related to the research of anticipation disorders in various mental disorders remain not fully studied, and it seems that there are no comprehensive studies that allow us to judge the relationship between the features of prediction disorders and specific nosology of neurotic disorders.
The purpose of this work was to study the features of antipathy abilities and coping strategies using patients with adaptive reaction disorder in the framework of neurotic and stress-related disorders as examples.
MATERIALS AND METHODS
Clinical–psychopathological and experimental–psychological research methods were used. (V.D. Mendelevich’s test of anticipation, L.A. Regush’s “Ability to predict” test, Lazarus’ coping test, clinical questionnaire for the identification and evaluation of neurotic states.)7–10 When applying statistical data processing, the program “IBM SPSS Statistics 25” was used. The following methods were used: descriptive characteristics (mean [M], standard deviation, confidence interval, median [Me], interquartile range [IQR] of the fraction), Shapiro–Wilk criterion (to determine compliance with the normal distribution of quantitative parameters), Pearson’s chi-squared test, Fisher’s exact criterion, Student’s t-criterion, Mann–Whitney U criterion, Kruskal–Wallis H criterion, Pearson correlation, Spearman’s correlation, diagrams: columnar and span.
The study involved 29 patients, (25 women [86.2%] and 4 men [13.8%]) with a diagnosis of “adaptive reaction disorder” from the ICD-10 section “Neurotic and stress-related disorders” (F43.2) between the ages of 20 and 60. All patients were treated in the day hospital of the Republican Clinical Psychiatric Hospital (Kazan).
RESULTS
The psych traumatic situations indicated by the patients were as follows: death or news of the illness of close relatives, dismissal from work, and conflicts in the family. The patients were characterized by symptoms of anxiety and depression such as depressed mood, anxiety, loss of interest in previously attractive activities, and sleep disorders. These symptoms were closely related to the traumatic event and developed within a month after that.
In accordance with the anticipatory concept of neurosis,5,6 the severity and surprise of the event that has become psych traumatic play a significant etiopathogenetic role in the formation of neurotic disorders. Within the framework of this study, this issue was studied in a targeted manner. It turned out that acute psychological trauma occurred before the mental disorder in 48.3% of patients, subacute in 44.8% and chronic in 6.9%. The majority of the examined revealed an unexpected psychological trauma (75.9% of cases), while the rest (24.1%) expected the psychological trauma.
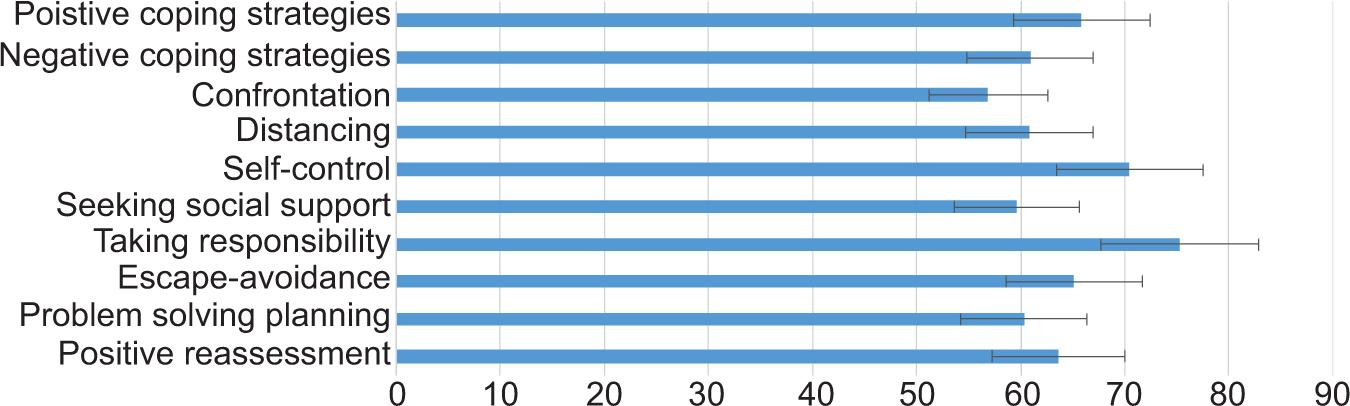
Experimental psychological examination showed that according to the test for the ability to predict L.A. Regush, a high level was determined in 4 subjects (13.8%), average in 23 (79.3%), and low in 2 (6.9%); according to the test of the “Coping Strategy” by R. Lazarus, it was found that negative coping strategies prevailed among nine respondents (31%). The main share among patients in this group belonged to the “taking responsibility” strategy; the “confrontation” strategy was less developed (Figure 1).
FIGURE 1. Average values of the “Coping Strategy” questionnaire test (R. Lazarus) in a group of patients with adaptive reaction disorder.
The results of the predictive competence test are shown in Figure 2. The test results showed that 6.9% of the surveyed (2 people) had general anticipatory insolvency, and 10.3% (3 people) had personality-situational insolvency. At the same time, spatial insolvency was detected in the majority of the surveyed, that is 69% (20 people), and temporary insolvency was detected in a third of the survey population (31%, 9 people).
FIGURE 2 . Average values of the test of anticipation consistency in the study group of patients.

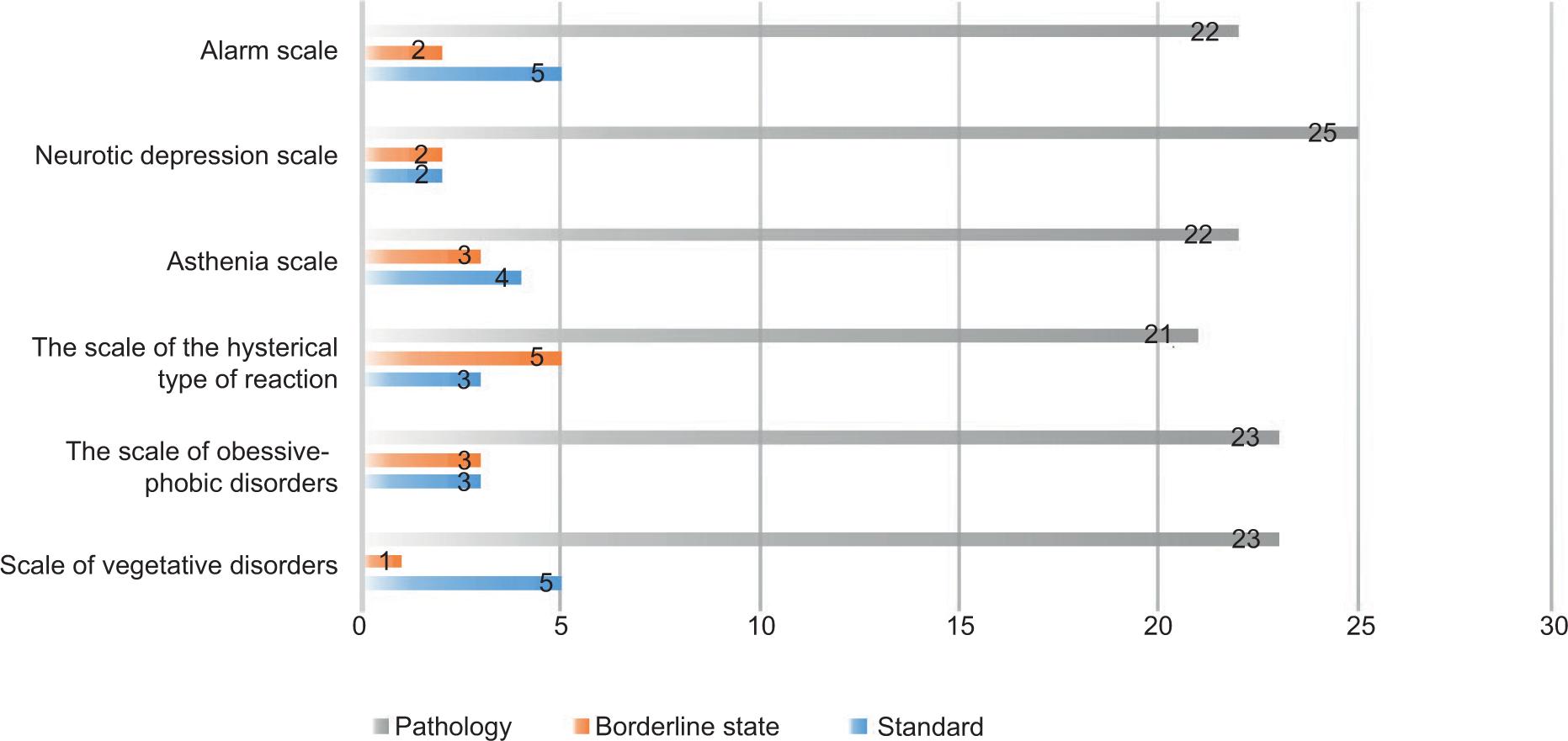
The data on the test for the detection and evaluation of neurotic states are shown in Figure 3. In the group of patients with adaptive reaction disorder, deviations were observed on all scales: on the anxiety scale (75.9%), neurotic depression scale (86.2%), asthenia scale (75.9%), hysterical response scale (72.4%), scale of obsessive-phobic disorders (79.3%), and the scale of vegetative disorders (79.3%).
FIGURE 3. Test data for the identification and evaluation of neurotic conditions in a group of patients with adaptive reaction disorder.
Based on the correlation analysis carried out, several numbers of relationships between the test indicators were revealed, the overall picture is shown in Figures 4 and 5, where the dotted lines reflect negative relationships, and the continuous lines reflect positive ones.
FIGURE 4. The correlogram of the studied indicators. The Cipher of Indicators: PS1, Psychological trauma 1 (severity index); PS2, Psychological trauma 2 (indicator of the nature of expectation/surprise); DB, duration of illness; Vzrt, age; UpC, ability to predict; K-I, confrontation; D-e, distancing; S-l, self-control; PSS, search for social support; PO, taking responsibility; B-I, escape-avoidance; PRP, planning a solution to the problem; PP, positive reassessment; OAS, general anticipatory solvency; CAC, personal-situational anticipatory solvency; PAS, spatial anticipatory solvency; VAS, temporal anticipatory solvency; PC, Anxiety scale; SHND, the Scale of neurotic depression; SHA, the Scale of asthenia; SHITR, the Scale of the hysterical type of reaction; SHOFN, the Scale of obsessive-phobic disorders; SHVN, the scale of vegetative disorders.
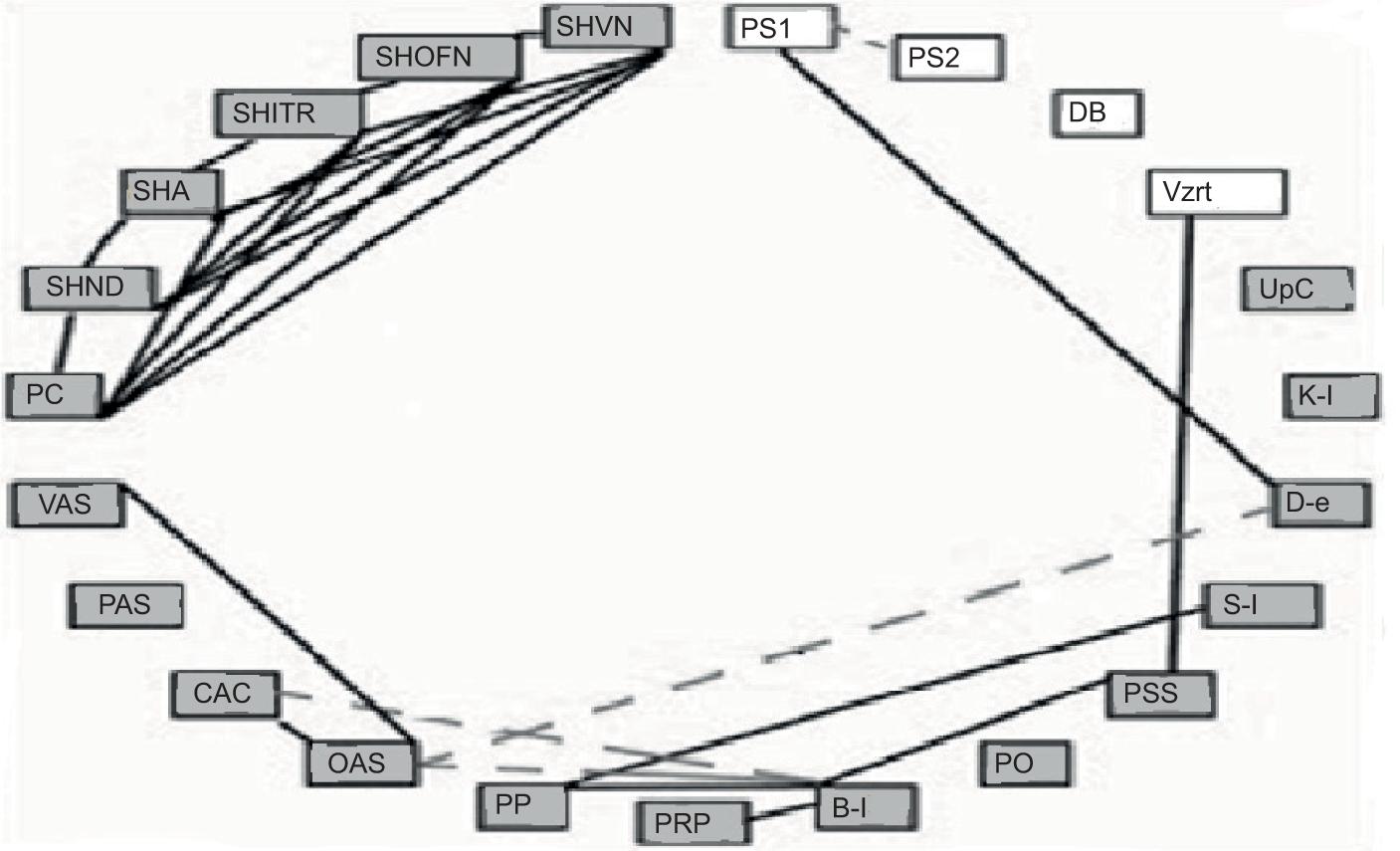
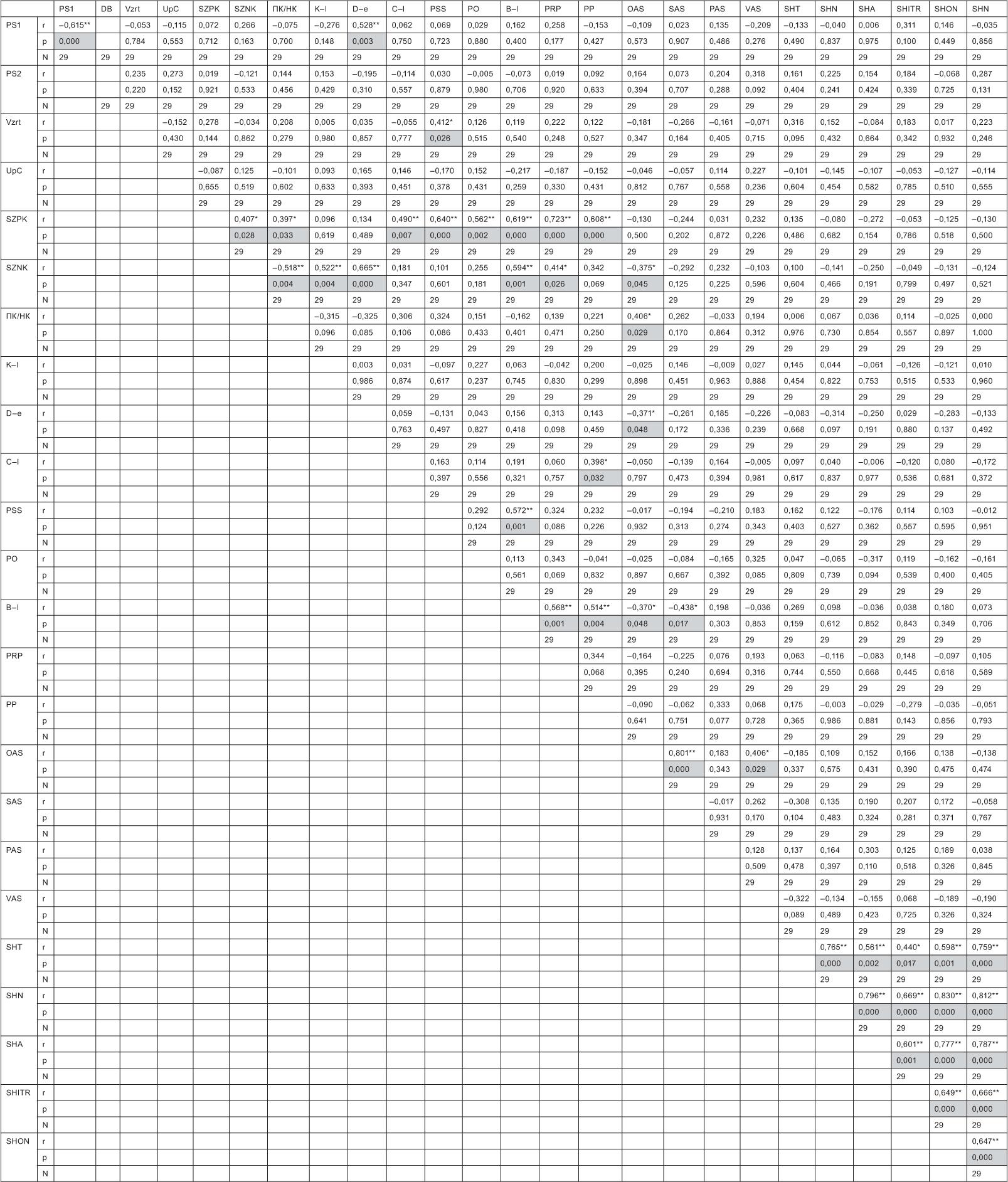
FIGURE 5. Correlation matrix of indicators in the group “Short-term depressive reaction due to adaptation disorder.” Cipher of Indicators: PS1, Psychological trauma 1 (severity index); PS2, Psychological trauma 2 (indicator of the nature of expectation/surprise); DB, duration of illness; Vzrt, age; UpC, ability to predict; SZPK, the average value of positive coping strategies; SZNK, the average value of negative coping strategies; K-I, confrontation; D-e, distancing; S-l, self-control; PSS, search for social support; PO, taking responsibility; B-I, escape-avoidance; PRP, planning a solution to the problem; PP, positive reassessment; OAS, general anticipatory solvency; CAC, personal-situational anticipatory solvency; PAS, spatial anticipatory solvency; VAS, temporal anticipatory solvency; PC, Anxiety scale; SHND, the Scale of neurotic depression; SHA, the Scale of asthenia; SHITR, the Scale of the hysterical type of reaction; SHOFN, the Scale of obsessive-phobic disorders; SHVN, the scale of vegetative disorders.
DISCUSSIONS
The psychological trauma index 1 has a direct correlation with the coping strategy “distancing” (P = 0.003, r = 0.528) and inverse correlation with the psych trauma index 2 (P = 0.000, r = −0.615). That is, “distancing” will be developed more strongly with the chronic nature of psychological trauma, and, in turn, acute psych trauma is more often unexpected. This kind of disorder was also observed during the COVID-19 pandemic in some countries.11,12
The older the patients with adaptive reaction disorder, the more they have developed the method of protection “search for social support,” because there is a significant positive correlation (P = 0.026, r = 0.412).
In this group, there are several direct interdependencies between the indicators of basic coping strategies diagnosed by the method of R. Lazarus. “Acceptance of responsibility” and “confrontation” stand apart, which do not correlate with any of the studied clinical, psychopathological, and path psychological indicators. There are four direct internal correlations in total. It was revealed that among patients of this group, the presence of consistency in general anticipation reduces the severity of the coping strategies “distancing” (P = 0.048, r = −0.371) and “escape-avoidance,” (P = 0.048, r = −0.370) the development of the latter method of protection also reduces personal situational prognostic competence (P = 0.017, r = −0.438).
Among the indicators of predictive competence, statistically significant direct correlations between general and personal-situational (P = 0.000, r = 0.801), general and temporary anticipatory abilities (P = 0.029, r = 0.406) were revealed.
The values of diagnostic coefficients on the scales of neurotic states have many internal reliable direct correlations, reflecting the interdependence of these signs in patients with a short-term depressive reaction due to an adaptation disorder, and the absence of such with other studied parameters. There are 15 internal direct correlations. This finding agreed with that of Kawabata and Onishi,13 who studied moderating effects of relational interdependence on depressive symptoms.
CONCLUSION
It can be stated that in patients with adaptive reactions disorder, personality-situational, spatial, and temporal insolvency, deviations from the norm on the scale of neurotic depression, the scale of obsessive-phobic and vegetative disorders, the scale of asthenia, anxiety, and the scale of the hysterical type of reaction were revealed. It was revealed that with the chronic nature of psychological trauma, the coping strategy “distancing” is more developed; with age, the method of protection “search for social support” becomes more pronounced in patients of this group. Correlations between anticipatory abilities and coping strategies were found; the presence of consistency in general anticipation reduces the severity of the coping strategies “distancing” and “escape-avoidance,” the development of the latter method of protection also reduces personal-situational prognostic competence, that is, patients with anticipatory consistency are less likely to use nonconstructive coping strategies, which, in turn, indicates the mutual influence of these functions.