INTRODUCTION
Dental caries is an irreversible microbial disease affecting the hard tissues of the tooth, and its manifestation persists throughout life even after the treatment. It affects all genders, social class, and all age groups, though children are affected more than the adult population.1,2 The World Health Organization (WHO) reported that 60–90% of children are affected by dental caries.3 According to the American Academy of Pediatric Dentistry (AAPD), dental caries in infants and children aged 71 months or below is known as early childhood caries (ECC) and is defined as the presence of one or more decayed teeth (non-cavitated or cavitated lesions), missing tooth due to caries, or filled tooth surfaces in any primary tooth.4,5 Dental caries is a global oral health burden affecting the overall health and quality of life,6,7 especially in underprivileged countries.1,8,9
Dental caries is an infectious disease induced by diet, cariogenic bacteria, fermentable carbohydrates, a susceptible tooth (host), and time.10 According to a report by the WHO, 530 million children were affected by dental caries of primary teeth3. The ECC prevalence differs among different population. In Far-east Asian countries, the prevalence was found to be 36 to 85% in the 3-years’ age group. In India, ECC prevalence has been reported as 44% in the age group of 8–48 months.11–13
In Middle East region countries, limited number of studies have been conducted on the prevalence and risk factors of ECC in the 0–6-years age group. Therefore, further studies to understand the prevalence and associated risk factors of ECC are required for the Middle East region. Most of the studies were done in the Kingdom of Saudi Arabia (KSA) and The United Arab Emirates (UAE) to assess the national prevalence of dental caries, which was high in preschool children. A study conducted by Al Agili reported 80% prevalence for primary dentition in the KSA, while another survey reported 83% prevalence for primary dentition among 5-year-old children in UAE.1,7 Another report found very high prevalence of dental caries in preschool children in UAE, from 36 to 47% in 2-year olds, 71–86% among 4-year olds, and 82–94% in 5-year olds.14 The reported prevalence from Ajman, UAE, and the western region were 71 and 93%, respectively.7
Therefore, the present systematic review was done to find the overall prevalence and associated risk factors in the 0–6-years age group in the Middle East region.
METHODS
A systematic literature search was performed to identify the articles on the prevalence and risk factors of early childhood dental caries for the 0–6-years age group in the Middle East region. The countries covered were Bahrain, the KSA, Kuwait, Oman, Qatar, and the UAE. The inclusion criteria were all literature published in English language from January 1, 1960 to December 31, 2020 for the 0–6-years age group. All preschool children in the age group of 0–6 years without any restriction to gender and socioeconomic status from applicable geographical location were included.
Search strategy
Three electronic databases PubMed, Cochrane, and Web of Science were searched for reviews of the existing studies. The keywords used for the searches were “children, infant, preschool child, dental caries, prevalence, and risk factors.” A comprehensive search strategy was developed and performed to search for relevant articles. The search strategy for PubMed was as follows: ((Children OR infant OR Preschool Child) AND Dental Caries AND (Prevalence OR “risk factor”)) “dental caries,” “preschool child,” “infant,” and “risk factors (“infant” [MeSH terms] OR “infant”[all fields]) OR ((“child”[MeSH terms] OR “child”[all fields] AND preschool [all fields]) OR (“child”[MeSH terms] OR “children”[all fields])) AND (“dental caries”[MeSH terms] OR (“dental”[all fields] AND “caries”[all fields]) OR “dental caries”[all fields]) AND (“risk factors”[MeSH terms] OR (“risk”[all fields] AND “factors”[all fields]) OR “risk factors”[all fields] OR (“risk”[all fields] AND “factor”[all fields]) OR “risk factor”[all fields] OR “prevalence”[all fields]) AND (“Saudi Arabia”[All Fields] OR “qatar”[MeSH Terms] OR “qatar”[All Fields] OR “qatar s”[All Fields] OR “UAE”[All Fields] OR “oman”[MeSH Terms] OR “oman”[All Fields] OR “kuwait”[MeSH Terms] OR “kuwait”[All Fields] OR “kuwait s”[All Fields] OR “bahrain”[MeSH Terms] OR “bahrain”[All Fields]) AND (1960:2020[pdat]). The search strategy for Web of Science was as follows: ((TS = infant) OR (TS = child) OR (TS = preschool) OR (TS = children)) AND ((TS = dental caries) OR ((TS = dental) AND (TS = caries))) AND ((TS = “risk factors”) OR ((TS = risk) AND (TS = factors)) OR (TS = prevalence)). The search strategy for Cochrane database was: “Children AND Prevalence AND Dental Caries.” The reference lists of existing systematic and other reviews were also explored for any other relevant and missed articles.
Selection process
The search was conducted on specified electronic databases by one investigator, and initially the related studies were selected using the keywords, title, and abstract. The duplicate studies were removed with the help of a reference management system (Mendeley Desktop). Afterward, two reviewers independently retrieved and reviewed all the selected studies. Initial screening was done at the level of title and abstract of the articles followed by the full-text screening of the selected articles to determine the eligibility for the present systematic review. The studies having age overlap, such as 5–7 and 6–12, were discussed among the reviewers, and studies wherein data on the 0–6-years age group were explicitly presented were included in our study. The two reviewers then shared notes, and disagreement on the inclusion and exclusion of any study was first resolved by mutual understanding or if required with the help of a subject matter expert.
RESULTS
Study selection and study characteristics
A total of 26 most relevant articles were included in the systematic review. The complete identification and selection process was depicted with the help of the PRISMA – 2020 (Figure 1). The main reasons for the exclusion of articles were the different outcome, study design, study setting, unsuitable age of the study population, non-availability of separate data on age group 0–6 years, and study location. The selected 26 full-text articles with a study population of 14,479, age group 0–6 years were included in the review. Table 1 shows the summary of extracted data from all the studies included in this review. The data table consisted of author or authors, year of publication, country, journal name, study setting, age, sample size, mean decayed missing filled teeth (DMFT), and prevalence. The data from four countries, namely the KSA, Kuwait, Qatar, and the UAE, were included in the study. The maximum number of studies belonged to the KSA (17 studies included), followed by the UAE (6 studies), Kuwait (2 studies), and Qatar (1 study). Out of 17 studies included from different parts of KSA, 6 were conducted in Jeddah, 4 in Riyadh, 2 each in Al-Kharj and Tabuk, and 1 each in Al-Ahsa and Al-Jouf, the northern region of KSA. The maximum number of studies were from Ajman (3) in UAE, followed by one each from Ras Al-Khaimah and Abu Dhabi. One study from UAE covered nine medical districts of UAE, namely Abu Dhabi, Al-Ain, western region, Dubai, Sharjah, Ajman, Um Al-Quwain, Ras Al-Khaimah, and Fujairah. Based on inclusion criteria, none of the publications could qualify for our study from Bahrain. The three articles found for Oman did not qualify to be included in the present study due to inappropriate age group.
FIGURE 1. Identification and selection process—PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) diagram.
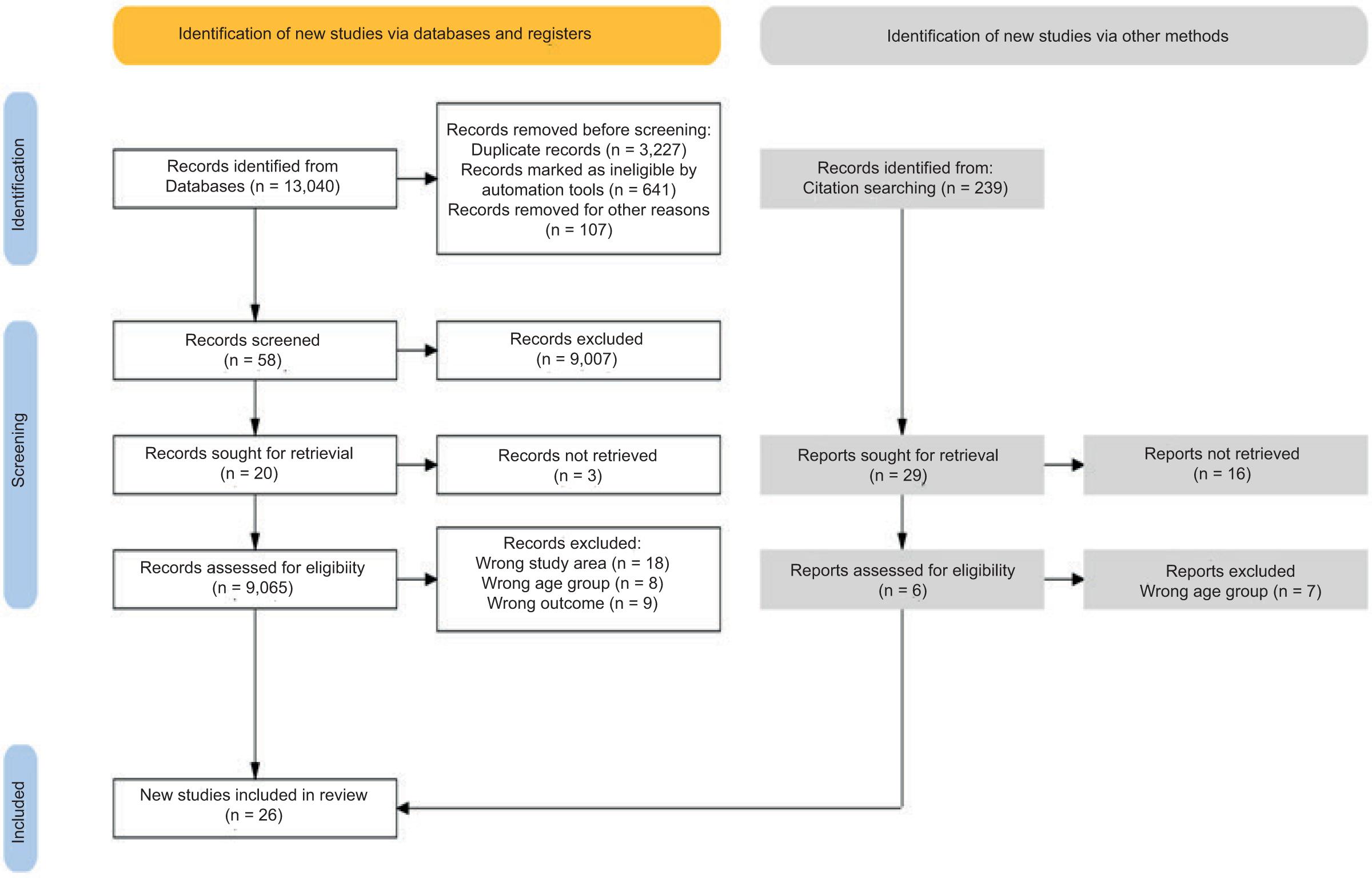
TABLE 1. Studies reported on prevalence of early dental caries among children from Middle Eastern region.
| Authors and Year | Country | Age (Years) | Sample | Mean DMFT | Prevalence (%) |
|---|---|---|---|---|---|
| Salem & Holm, 198515 | Saudi Arabia | 3–5 | 296 | 1.2 | 33.40 |
| Al-Mohammadi et al., 199716 | 2, 4, 6+ | 396 | 2+ years: 1.83, 4+ years: 3.86 |
45.66 | |
| Paul & Maktabi, 199717 | 5 | 103 | 7.12 | 83.50 | |
| Al-Banyan et al., 200018 |
5–12 | 272 | 5 years: 4.5, 6 years: 4.3 |
99 | |
| Al-Malik & Holt, 200019 | 4–5 | 80 | 0.95 | 30 | |
| Stewart et al., 200020 | 5–15 | 114 | 7.66 | 92.5 | |
| Al-Malik et al., 200121 | 2–5 | 987 | - | 73 | |
| Wyne et al., 200122 | 2–6 | 1016 | 8.6 | 27.30 | |
| Al-Malik et al., 200223 | 2–5 | 987 | - | 73 | |
| Wyne, 200824 | 3–5 | 322 | 2.92 | 62.70 | |
| Al-Malik et al., 200325 | 2–5 | 987 | 4.8 | 73 | |
| Paul, 200326 | 5 | 103 | 7.1 | 83.50 | |
| Sabbah et al., 200327 | 1–5 | 574 | 1.17 | 26.50 | |
| Wyne, 200824 | 3–5 | 789 | 6.1 | 74.80 | |
| Farsi et al., 201328 | 4–5 | 407 | - | 65 | |
| Al-Meedani & Al-Dlaigan, 201629 | 3–5 | 388 | 3.4 | 69 | |
| Gudipaneni, 201930 | >5 | 270 | - | ||
| Murtomaa et al., 199531 | Kuwait | 3–7 | 382 | 4.22 | 58.63 |
| Al-Mutawa et al., 201032 | 5–14 | 714 | 4.6 | 85.6 | |
| Alkhtib et al., 201633 | Qatar | 4–5 | 250 | 7.66 | 89.20 |
| Hashim et al., 200634 | The United Arab Emirates | 5 or 6 | 1036 | 4.4 | 76.10 |
| Hashim et al., 200935 | 5 or 6 | 1036 | 45 | ||
| El-Nadeef et al., 20097 | 5 | 1340 | 5.1 | 83 | |
| Hashim et al., 201036 | 5–6 | 1036 | 4.5 | 76.40 | |
| Kowash et al., 201737 | 4–6 | 540 | 3.07 | 74.10 | |
| Elamin et al., 20186 | 18–4 | 186 | 1.7 | 41 |
DMFT, decayed missing filled teeth.
Most of the studies were carried out in pre-, primary, and nursery schools, kindergartens, and other places such as in health or dental clinics and outpatient departments (Table 1). The earlier and latest studies included in our review were conducted in 1985 by Salem and Holm in Gizan and Gudipaneni in northern Saudi Arabia.30 In 1985, Salem and Holm reported 33.40% ECC prevalence with a mean DMFT of 1.2 among children aged 3–5 years.15 The country-wise prevalence with mean DMFT values is provided in Table 1. The study setting and dental caries diagnostic criteria of finally available studies are shown in Table 2. The analysis revealed that ECC prevalence ranged from 26.50 to 99% in the Middle East region. The highest ECC prevalence of 99% was reported by Al-Banyan et al. in their study conducted in Riyadh, KSA in 2000.18 They further mentioned that among all groups, only 0.7% had no caries experience. The lowest prevalence was reported as 26.50% with a mean DMFT of 1.17 by Sabbah and Stewart in a study conducted in Tabuk, Saudi Arabia among children aged 1–5 years.27 The mean DMFT ranged from 0.95 to 16.9, which was reported in studies from Jeddah, West Province, and Al-Jouf, northern region of Saudi Arabia.19,30 In the UAE, the prevalence ranged from 41 to 83%.6,7 A national survey conducted by El-Nadeef et al. on the oral health of 5-year-old children in nine medical districts of the UAE reported the highest prevalence of 83%.7 Two studies including one each from the KSA and the UAE did not mention the ECC prevalence. Country-wise latest study included in this review was conducted in 2018 in Abu Dhabi, UAE by Elamin et al., which revealed 41% ECC prevalence in that part of the UAE.6 The included studies covered a minimum age of 1 year.27
TABLE 2. Study setting and diagnostic criteria used in the finally available studies.
| Author, Year | Country | Study setting | Diagnostic criteria and instrument |
|---|---|---|---|
| Salem & Holm, 198515 | Saudi Arabia | Hospital | WHO, Mouth mirror, probe |
| Al-Mohammadi et al., 199716 | Dental clinic | WHO criteria | |
| Paul & Maktabi, 199717 | Nursery | WHO, Mirror, probe, dental light | |
| Al-Banyan et al., 200018 | School | Haugejorden, Dental explorer | |
| Al-Malik & Holt, 200019 | School classroom | BASCD, Plane mouth mirror, Daray “Versaule” light | |
| Stewart et al., 200020 | Clinic | WHO, probe, mouth mirror, dental unit light | |
| Al-Malik et al., 200121 | Kindergarten | BASCD, Plane mouth mirror, Daray “Versaule” light | |
| Wyne et al., 200122 | Preschool | WHO, Mirror, explorer, fiber optic light source | |
| Al-Malik et al., 200223 | Kindergarten school | BASCD, Plane mouth mirror, Daray light | |
| Wyne, 200824 | Preschool | WHO, Disposable mirror heads, probe, natural light | |
| Al-Malik et al., 200325 | Nursery school | WHO, Mouth mirror, Daray light | |
| Paul, 200326 | Nursery | WHO, Plane mouth mirror, Daray light | |
| Sabbah et al., 200327 | Clinic/Hospital | WHO | |
| Wyne, 200824 | Preschool | WHO | |
| Farsi et al., 201328 | Nursery school | WHO, Mouth mirror, community periodontal index probe, pen light | |
| Al-Meedani & Al-Dlaigan, 201629 | Kindergarten school | WHO, 1997, Disposable examination kits, portable light | |
| Gudipaneni, 201930 | OPD dental clinic | WHO, Disposable mouth mirror, artificial light | |
| Murtomaa et al., 199531 | Kuwait | Kindergarten and primary school | WHO, Disposable mouth mirror and explorer |
| Al-Mutawa et al., 2010 32 | School dental clinic/School health room | WHO, 1997, Mouth mirror, WHO ball tip probe | |
| Alkhtib et al., 2016 33 | Qatar | Kindergarten | WHO, Disposable mouth mirror with fiber optic light |
| Hashim et al., 2006 34 | The United Arab Emirates | School health clinic | WHO, Disposable mouth mirror, natural day light |
| Hashim et al., 2009 35 | School health clinic | WHO, Disposable mouth mirror, natural day light | |
| El-Nadeef et al., 20097 | School | WHO, Mouth mirror, blunt explorer | |
| Hashim et al., 201036 | School health clinic | WHO, 1997, Disposable mouth mirror, natural day light | |
| Kowash et al., 201737 | Preschool | WHO, 1997, Mouth mirror, torch light | |
| Elamin et al., 20186 | Nursery school | WHO, Mouth mirror, blunt ball-ended probe |
BASCD, British Association for the Study of Community Dentistry; OPD, outpatient departments.
Risk factors
An extensive range of exposures was studied in the included studies. The information on the exposures was obtained from the caregivers of the child, mainly from one of the parents through a questionnaire. Information regarding socioeconomic background, demographic data, oral hygiene and dental practices, feeding history, dietary habits, and other factors were examined in the studies. These risk factors were categorized as sociodemographic factors, dietary factors, oral hygiene practices, feeding practices, oral bacteria, and healthcare system–related factors. The evaluation of the included studies revealed a total number of 103 risk factors for ECC among the 0–6 age group, which were explored by 26 studies. Among them, 16 were related to the sociodemographic status, 28 to dietary habits, 21 to oral or dental hygiene practices, 17 were related to the healthcare system, and 21 were grouped under other varied factors. The summary of the risk factors included in all studies has been provided in Table 3.38
TABLE 3. List of the potential risk factors: Early childhood caries in children, age group 0–6 years.
| Factor | Details |
|---|---|
| Sociodemographic factors | Age of the child (higher in older children) Low socioeconomic group or class Low educational levels Parent’s education Mother’s low educational level Lower professional families Low-income family Family size Type of school (publicly funded) Rural nursery location, Barriers to dental care services Parents’ busy lifestyle Gender (Females were more likely to have enamel defects and/or deep fissures than males which put them at higher risk for caries) Gender (males) Traditional practice of overindulging sons in Arabic culture Ethnicity: Emirati nationality (local) children |
| Dietary factors | Sweetened snacks and drinks High consumption of cariogenic food Increased availability of sweetened snacks and drinks Increased use of sweetened snacks and drinks High consumption of sugary foods and beverages between normal meals Consumption of carbonated drinks and fruit syrups Consumption of carbonated (fizzy) drinks daily, and at bedtime Children having packed fruit juice (cartons) Consumption of dates once daily or more often than other fruits Dummy dipped in honey or sugar Consumption of diluted fruit syrup during early years Frequency of use of diluted fruit syrup drinks at the time of survey Consumption of pure fruit juices at the time of the survey Cariogenic food habits Lack of dietary discipline Sugar consumption (frequent high sugar intake) Easy access and recurring exposure to cariogenic foods and drinks High accessibility of snacks Eating habits of children Sugar consumption in the form of snacks Irregular meal patterns Reduced ability to control children’s diet High consumption of cariogenic foods in school children High consumption of refined sugars by children Frequent snacking between meals (3 or more times per day) Cariogenic snack consumption 3 or more times a day—Confectionery (chocolates, candies, and jellybeans) Frozen confectionery High consumption of sugary tea |
| Oral hygiene practices | Poor oral hygiene practices Lack of oral hygiene practices Late starting age for infant tooth cleaning Brushing occasionally Late starting of brushing habit (over 1 year) Child brush teeth alone without assistance Lack of oral hygiene discipline Delayed first dental visit for routine checkup Poor interest in dental care by the parents Children never visiting a dentist Poor dental behaviors Poor dental attitudes Irregular dental visits Frequency of tooth brushing Parents’ dental knowledge and attitude toward their own dental health Lack of oral care awareness in the parents Widespread neglect of the oral health Absence of oral health awareness among parents Lack of routine dental care Visible plaque Infrequent tooth brushing |
| Healthcare system– related factors | Scarcity of trained dental healthcare professionals Low dentist/population ratios Lack of interest in the specialty from Saudi graduates Lack of immediate and visible results of preventive programs Dentists posting to isolated areas on temporary assignments Nonavailability of conventional dental setup Remote villages Nursing care pattern Increasing cost of dental treatment Limited accessibility and availability of dental services Large unmet treatment needs Less emphasis on preventive care (dental) Unevenness in the distribution of program resources Discontinuation of water fluoridation program Lack of an effective fluoridation policy Inadequate oral healthcare system Lack of access to professional dental care |
| Others | Major decay component Untreated decayed teeth Lack of dental health knowledge Low water fluoridation Drinking non-fluoridated tap water Previous caries experience Staining in pits and fissures |
| Enamel demineralization Older sibling having caries Presence of oral bacterial flora mutans streptococci Presence of developmental enamel defects Complex morphological nature of posterior teeth Lack of community awareness and understanding about prevention and treatment of caries Parental indifference and belief that primary teeth are replaceable by permanent teeth Subsidies for sugar production and use Presence of fluoride in drinking water Feeding practices—Wholly breastfed Timing: Fruit syrup in a feeding bottle at bedtime/nap time during early years Infant feeding practice Nursing bottle caries |
Most studies found low socioeconomic status, gender, age of the child, parents’ education, low maternal education, and type of school to be significant factors for the development of ECC. Children attending public schools were at a greater risk of having ECC. Gender (male) was another important risk factor for ECC. Two studies mentioned that the reason could be the widespread traditional practice of overindulging sons in Arabic culture. Other factors explored by studies were location, parents’ busy lifestyle, and Emirati nationality.
Out of 28 dietary factors associated with ECC, consumption of sweetened snacks and drinks, frequent consumption, easy access, and availability, frequent snacking between meals (3 or more per day), and a lack of dietary discipline were the major reasons for the occurrence of ECC.38
Many studies revealed that poor or lack of oral hygiene practices, late starting age for tooth brushing habit (over 1 year), and lack of oral hygiene discipline were major risk factors for ECC.26,39–46 Among other factors, some studies revealed that parents’ poor interest and awareness in dental care and the attitude toward their dental health as factors responsible for widespread neglect of oral care, hence risk factors for early development of caries.26,38–46
Interestingly, some studies explored the role of healthcare system–related factors in the development of early dental caries. Studies also observed the scarcity of trained dental healthcare professionals, low dentist to population ratios, limited accessibility and availability of dental services, less emphasis on preventive care and nonavailability of conventional dental setup, and high cost of dental treatment, and discontinuation of water fluoridation program.47–49 A few studies stated the presence of major decay components and untreated decayed teeth, and low fluoride levels as the main risk factors for developing ECC.50–52 Other factors linked with ECC were lack of dental health knowledge and awareness about prevention and treatment of caries, previous caries experience, staining in pits and fissures, and enamel demineralization. Dental caries in older sibling was pointed out as a risk factor in one study. Other factors were the presence of developmental enamel defects and complex morphological nature of posterior teeth. The lack of awareness among parents also play a major role as due to the belief that primary teeth will eventually be replaced by permanent ones. Various studies revealed that the presence of mutans streptococci in children put them at a greater risk of developing dental caries.38,53–58
DISCUSSION
The present systematic review was attempted to determine the prevalence and risk factors of ECC in the Middle East region. Review of the eligible studies included in this study was helpful in determining the range of prevalence of ECC in this region. All the studies included in the review were assessed on quality using the Newcastle–Ottawa scale, a star rating system, in which the quality was determined based on the scoring. Some of the studies included the age groups 2, 4, and 6+ years, 3–7 years, and Grade 1 (5–7 years). In such cases, the study was included if the data related to 0–6 years of age were given explicitly, otherwise the study was excluded. Most of the studies (22 studies) used WHO’s diagnostic criteria; three used the British Association for the Study of Community Dentistry (BASCD), and one study followed the Haugejorden recommendation. Studies used DMFT index to measure ECC. Out of 26 studies included in this review, 22 studies used DMFT to measure ECC experience. The overall prevalence in the Middle East region cannot be generalized for the whole region because most of the studies included in the review were from the KSA (17), followed by the UAE (6), Kuwait (2), and Qatar (1).
Our review revealed 103 risk factors affecting the status of ECC among 0–6 years age group in the Middle East region. Low socioeconomic factors as well as healthcare system–related factors such as limited accessibility and availability of dental services and less emphasis on preventive dental care play an important role in the high development of dental caries in children.59-60 Additionally, other factors such as the parents’ approach and attitude toward their own dental care affect the dental care of the children too, as children in this age group are mostly dependent on their caregivers or parents.61 Similar findings have been indicated by Chen et al.62 in a systematic review on the global prevalence of ECC in a 5-year-old population published in 2018. Dietary factors were another significant reason for the increasing ECC in this age group. High consumption of sugary foods and beverages and poor oral hygiene have been associated with increased caries among children by other reviews too, and immediate attention is required by the government to reduce ECC.63-65 The presence of major decay components and untreated decayed teeth and low fluoride levels were other risk factors for developing ECC in children; hence, authorities should focus on these factors along with the above-mentioned factors to control the caries.66-68
The major limitation of this review was the incomplete representation from all relevant countries which limited us from the meta-analysis. No study publication from Bahrain could be found. Similarly, no suitable study as per our review requirement could be found for the Omani population. So, the result of this review cannot be generalized for the entire Middle East region. Further research should be conducted in the unreported countries and regions to predict the actual prevalence of ECC.
CONCLUSION
Present systematic review disclosed the need of government authorities across Middle East countries to focus on the increasing burden of ECC among preschool children. ECC is a preventable disease, hence, the rate of prevalence can be curtailed by focusing on prevention programs on dental caries, developing awareness-generating programs focusing on oral health education, and increasing access and availability of dental care services.